Crohn’s disease is a form of chronic inflammatory bowel disease (IBD) that prevails at one or more locations along the gastrointestinal (GI) tract. It affects both males and females equally, and is more prevalent in developed countries, Europe and North America than in other parts of the world. Patients with the disease may experience intermittent periods of flare-ups (when symptoms occur) and remission (when symptoms subside). Symptoms that lead to a diagnosis are usually observed in childhood or early adulthood (15 – 35 years of age, on average).
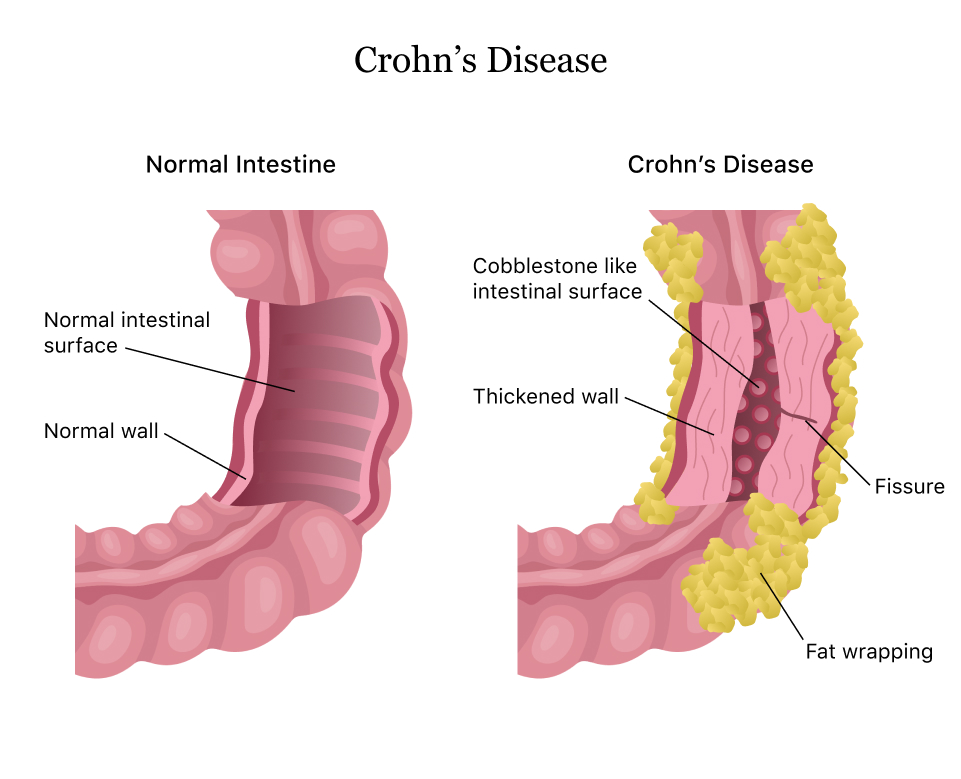
Image from Drugwatch
Symptoms
While symptoms may vary between patients, they usually include one or more of the following:
- diarrhoea that persists for more than seven days
- rectal bleeding (blood in stools)
- abdominal cramps and aches (often in lower right quadrant of stomach)
- urgency to pass stools
- feeling of incomplete bowel evacuation
- constipation, leading to bowel obstruction
Occasionally, a patient may additionally experience some of the following symptoms:
- fever
- nausea and/or vomiting
- joint aches or swellings
- mouth ulcers
- swollen, painful, red patches on the skin (mostly on the legs)
- sore, red eyes or vision changes
Complications
Some of the less severe complications that may be experienced with Crohn’s disease include:
- fatigue
- weight loss
- loss of appetite
- stunted or delayed growth in children
However, there are more severe complications that are associated with the disease including:
- fissures – tears in the tract lining that may cause pain and bleeding
- fistulas – formation of abnormal channels between one part of the intestine and another, or with the bladder, skin or vagina, resulting from inflammation
- strictures – narrowing of parts of the intestine, resulting from chronic inflammation
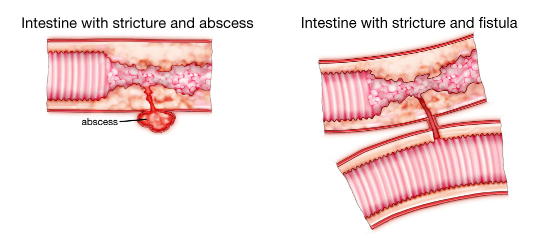
Image adapted from Trusted Therapies
These complications may subsequently cause other problems such as bowel damage or scarring that may require surgery, difficulty in absorbing nutrients from food (leading to conditions such as iron deficiency anaemia, osteoporosis) and bowel cancer.
Some medicines taken for Crohn’s disease may cause complications to the foetus during pregnancy, and should therefore be discussed immediately with your doctor. Flare-ups may also temporarily reduce fertility in women, while medication for Crohn’s disease may temporarily reduce fertility in men.
Causes
While diet and stress may play a role in the occurrence of flare-ups, they do not cause the disease itself. Research suggests that Crohn’s disease may be associated with the following aspects:
- autoimmunity – The individual’s immune system mistakes normal gut bacteria for foreign organisms and elicits an immune response to destroy them. The resulting inflammation persists without subsiding, resulting in chronic inflammation, ulceration, thickening of the gut wall and, subsequently, other symptoms that are outwardly experienced.
- family history – There appears to be a genetic link to the disease as about 5-20% of patients are found to have a close (first-degree) relative with the same condition.
- environmental factor – Although certainly not limited to these areas, Crohn’s disease appears to have a higher prevalence in developed countries, urban areas and countries in the Northern hemisphere.
Diagnosis
Since some of the symptoms of Crohn’s disease may be similar to those observed with more common (mostly bacterial) infections, your GP might need to take a closer look at your medical history, family history and all the symptoms observed. Initial testing would ideally involve:
- physical examination (touch and feel) of the abdomen
- laboratory tests on blood and stool samples – to test for infections or inflammation, the latter of which could be a result of Crohn’s disease
- X-rays of the GI tract, possibly with the aid of a contrast chemical
Following these, the patient may be referred to a specialist to carry out further testing that may include:
- upper endoscopy, where a camera is inserted through the mouth at the end of a light tube, allowing the doctor to observe the insides of the GI tract for inflammation; this allows examination up to the first part of the small intestine (duodenum)
- colonoscopy, where a camera is inserted through the anus, again to look for signs of inflammation; this allows examination of the large intestine
- chromoendoscopy, where a blue dye may be sprayed on the gut wall during a colonoscopy to detect slight changes in the gut wall
- biopsy, which involves nipping of tiny pieces of the gut wall in order to carry out pathological testing for Crohn’s disease (and even to screen for cancer)
- enterography – fluoroscopic X-ray, MRI scan or CT scan, which involves ingestion of a contrast dye that would allow the observation of abnormalities in the GI tract; this allows examination of areas that cannot be reached by endoscopy and colonoscopy
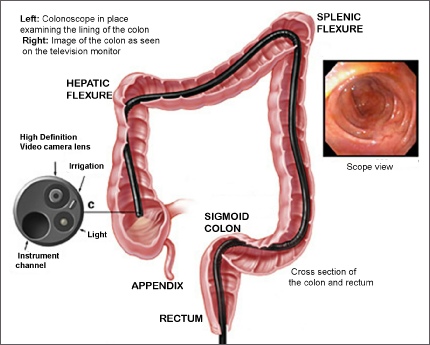
Image from Glasgow Colorectal Centre
Prevention
There is no means of preventing the incidence of the disease itself. However, careful observation and management may help to prevent flare-ups in some instances.
- While there are no specific dietary restrictions for Crohn’s disease, it is best to maintain a balanced, healthy diet that provides the required levels of nutrition and allows easy bowel movements. Some patients find that certain foods tend to trigger flare-ups. These should be noted and avoided to prevent worsening of symptoms.
- Children may sometimes need to be put on a well-rounded liquid diet to help reduce flare-ups.
- Stopping smoking has shown to reduce flare-ups in patients who previously smoked.
- Medical advice should always be sought prior to taking any other medication as some medicines, such as NSAIDs, can worsen symptoms.
- Medication used in the treatment of Crohn’s disease, such as immunosuppressants and other specific medicines, tend to increase the risk of infection. It is therefore recommended to receive the annual influenza vaccine as well as the pneumococcal (pneumonia) vaccine. However, avoid receiving live vaccines (e.g. MMR).
- It is also recommended that patients with Crohn’s disease get themselves screened for bowel cancer regularly as there is an increased risk as a result of bowel damage. The longer the condition has been prevalent, the higher the risk of bowel cancer.
Treatment
At present, there is no permanent cure for Crohn’s disease. However, there are several types of treatment that may be administered in order to control symptoms and flare-ups. These include:
- steroids – Usually taken orally, these may help to reduce inflammation – and therefore symptoms of Crohn’s disease. They are ideally prescribed for a couple of months and may have side effects such as weight gain, trouble sleeping, indigestion, increased risk of infection, wearing away of bones, reduced growth rate in children.
- immunosuppressants – These may be administered orally or by injection, and may be taken as a form of long-term treatment where steroids seem ineffective on their own. Long-term use may lead to increased risk of infection, nausea and/or vomiting, liver issues. Commonly used immunosuppressants include methotrexate, azathioprine and mercaptopurine.
- biological medicines – These are stronger medicines used in the event of other medication not being strong enough. They are usually administered via injection or drip every few weeks and may be taken for several months or years. Side effects may include an increased risk of infection, fever and joint aches. Commonly used biological medicines include infliximab, adalimumab, vedolizumab and ustekinumab.
- enteral nutrition – As mentioned earlier, it may be required for some children and young patients to be put on a liquid diet in order to control symptoms or flare-ups. This may be administered for a few weeks and involves specially prepared drinks containing all the required nutrients. Adverse effects are few and may include nausea, diarrhoea, constipation.
- resection surgery – In the event where it appears that medication is not having much effect, surgery may be recommended by your doctor. This usually involves removing a section of inflamed bowel using keyhole surgery, and reconnecting the remaining parts of the bowel. Recovery may take a few months, and an ileostomy (passing of stools into an externally attached pouch instead of through the anus) may be required in some cases until recovery is completed.
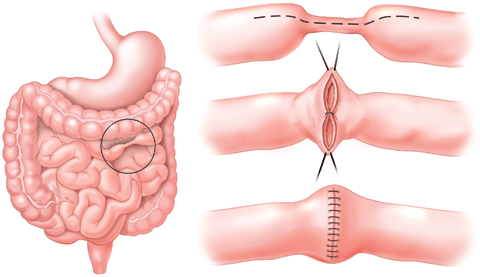
Image from Columbia University Department of Surgery
Cover illustration from Healthline

2 Comments Add yours