The inner lining of the uterus that is shed during menstruation every month is known as endometrium and the tissue present on this inner wall is called endometrial tissue. Endometriosis refers to the abnormal growth of endometrial tissue in areas outside of the uterus. This may manifest in different parts of the abdomen including:
- ovaries
- fallopian tubes
- outer surface of uterus
- uterosacral ligaments (ligaments that support uterus)
- anterior cul-de-sac (space between uterus and bladder)
- posterior cul-de-sac (space between uterus and rectum)
- pelvic cavity lining
Less commonly, endometrial tissue may also be found on the intestines, bladder, vagina, rectum, cervix, vulva or abdominal surgery scars.
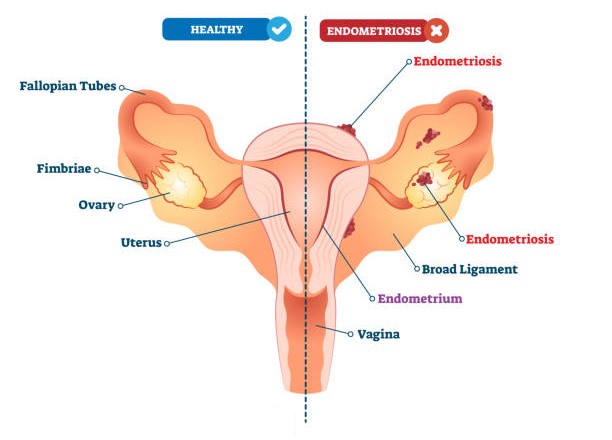
Image adapted from iStock
Every month, if fertilisation does not occur, the endometrium is shed at the start of the menstrual cycle, and later rebuilt in preparation for potential fertilisation in the next cycle. This process of breaking down and rebuilding of endometrial tissue is driven by varying levels of female reproductive hormones. In individuals with endometriosis, as each hormone goes through its path in a cycle, the endometrial tissue present outside the uterus also responds in the same way as the uterine endometrial tissue. Bleeding from extra-uterine endometrial tissue usually results in an inflammatory response, which causes the pain and cramps experienced by patients. This may also cause irritation and as scarring, which further contributes to the pain.
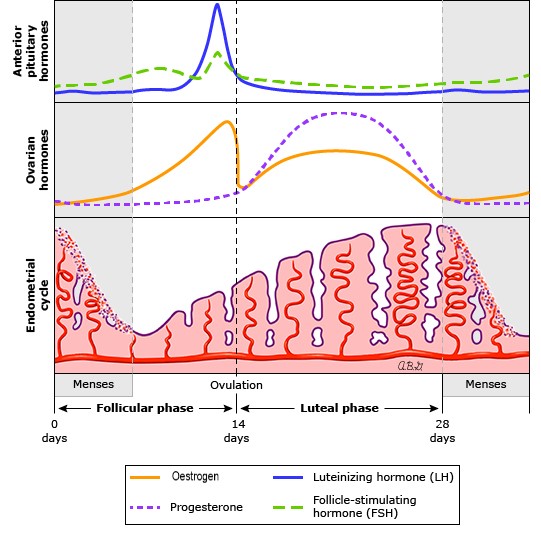
Image adapted from UpToDate
Endometriosis may be classified as minimal, mild, moderate or severe depending on the extent of tissue growth, damage to fallopian tubes, involvement of other pelvic organs and extent of adhesions. It is estimated that endometriosis affects around 10% of women of reproductive age.
Symptoms
Symptoms of endometriosis may vary from one individual to another, and are not necessarily indicative of how severe the condition is in an individual. That is, an individual with severe endometriosis may experience mild or no symptoms while another with mild endometriosis may experience severe symptoms. Such symptoms include:
- frequent pelvic pain (abdomen and lower back) that worsens during menstruation
- debilitating menstrual cramps that affect basic activity
- heavy or abnormal bleeding during menstruation
- pain during or after intercourse
- painful urination and/or bowel movements during menstruation
- nausea, diarrhoea or constipation during menstruation
Complications
The most significant complication that may arise with endometriosis is infertility. In fact, between 20-50% of women with fertility issues have been found to have endometriosis, so much so that infertility is sometimes referred to as a symptom (rather than a complication) of endometriosis. The principal cause of this is believed to be damage caused to the fallopian tubes and/or ovaries by endometriosis. This could subsequently distort the fallopian tubes’ function of picking up and transferring the released ovum (egg) to the uterus, or may impair the overall function of the ovaries, fallopian tubes, uterus or ovum.
In the case of infertility resulting from endometriosis, it is unlikely that medication could help the issue, and surgery to remove endometrial tissue might have limited results. In vitro fertilisation (IVF) may help in mild to moderate cases of endometriosis, but may be less effective in severe cases.
Other complications that may arise include adhesions, where sticky endometrial tissue may cause abdominal organs to adhere to one another, and ovarian cysts, which may become enlarged and painful over time. When endometriosis occurs within the ovaries and causes ovarian cysts, the condition is referred to as endometrioma. While surgery might be used to address both of these complications, it is highly likely that they would return in the future.
Endometriosis patients also often experience emotional distress that may arise as a result of the adverse symptoms and complications mentioned above and their hampering effect on everyday life.
Causes
It is not clear as to what exactly causes endometriosis, but scientists have come up with several plausible causes:
- retrograde / reverse menstruation – during menstruation, some endometrial lining may flow back up through the fallopian tubes and into the abdominal cavity where it may embed itself
- spread via bloodstream or lymphatic system – endometrial tissue may travel via these channels and embed themselves elsewhere in the body
- direct transplantation – following surgeries such as caesarean sections, endometrial tissue may be inadvertently directly transplanted in other areas such as the abdominal wall or scar tissue
- family history – women with closely related individuals who have suffered from endometriosis seem to be at a higher risk of developing the condition themselves
- immunity – it has been suggested that issues with an individual’s immune system may also contribute towards the incidence of endometriosis, although there is limited clarity with regard to the contribution of this factor
Diagnosis
While observation of the above-mentioned symptoms may strongly suggest the presence of endometriosis, a confirmed diagnosis is usually made by means of laparoscopy. During this procedure, a doctor would examine the internal cavity of the pelvic region for any abnormal tissue growth. Usually, if suspected endometrial tissue is observed, a biopsy would also be carried out to study the tissue microscopically and determine if it is indeed endometrial tissue.
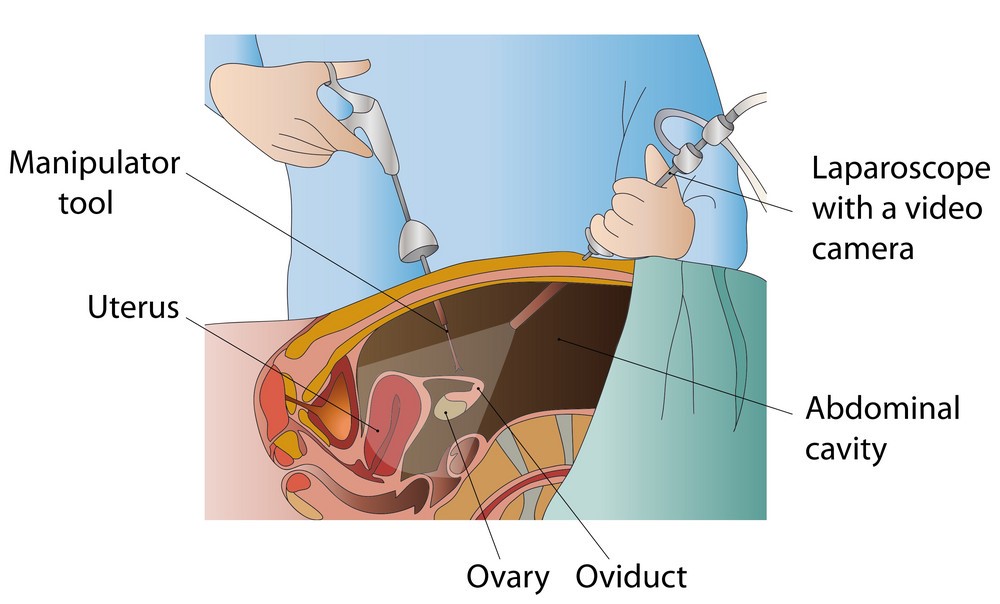
Image from VectorStock
Non-invasive ultrasound, CT or MRI scanning may be carried out prior to this in order to look for any possible abnormalities in the pelvic or abdominal region.
Prevention
There is no means of preventing the incidence of endometriosis.
Treatment
There is no known cure for endometriosis as yet. However, treatment may help to alleviate symptoms, slow tissue growth or potentially improve fertility in some cases. Prior to deciding on which treatment should be followed, it is imperative to have a discussion with your doctor, taking into consideration your age, symptoms, plans for pregnancy, as well as the side-effects and after-effects of surgery and other available options. Some modes of treatment that might be discussed include:
- pain management – NSAIDs may be administered in order to control inflammation and pain
- hormone therapy – depending on the individual’s condition, a doctor may administer the oral contraceptive pill (contains both oestrogen and progestin and may help to reduce menstrual flow), progestin-only pill, gonadotrophin-releasing hormone (GnRH) agonist (to induce a temporary ‘medical menopause’), danazol (a testosterone derivative); hormone therapy could cause several side-effects and therefore needs to be carefully discussed with a doctor prior to commencement
- laparoscopic surgery – to remove endometrial tissue (and even ovarian cysts) by excision or fulguration (burning); again, this needs to be carefully talked through with a doctor first – there is no guarantee that regrowth will not occur
- hysterectomy – major surgery for removal of the uterus; the ovaries may also be removed in some instances, in which case the patient would subsequently need to get on hormone replacement therapy (HRT) – there is no guarantee that regrowth will not occur
Given the intense nature of most forms of treatment for endometriosis, it is generally recommended that symptoms be observed over a period of time first as in some cases, endometriosis naturally subsides over time. However, this should be monitored closely as in some other cases, symptoms may worsen if left untreated.
Illustration from American Chemical Society
