The sciatic nerve has the largest diameter of all the nerves in the human body. It originates in the lower spinal cord and extends all the way down through the hip, buttock and posterior part of the thigh before branching out above the knee joint and continuing down to the foot.
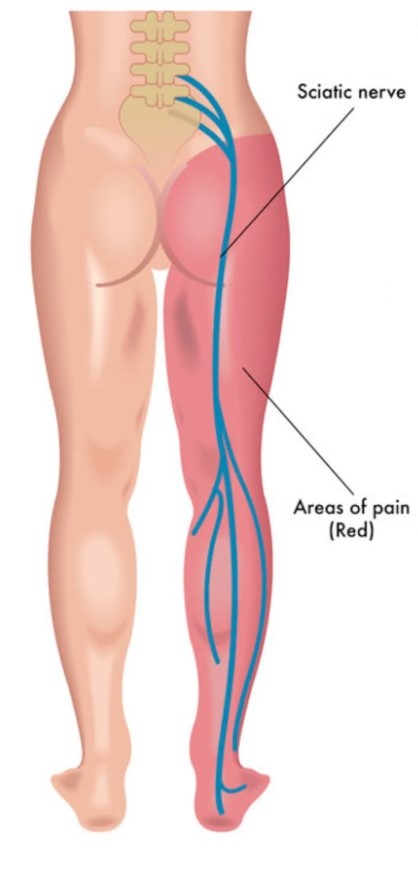
Illustration adapted from HealthCare
Sciatica is not a medical condition itself, but a symptom that arises as a result of the sciatic nerve being irritated, compressed or inflamed. On average, sciatica could last for between four to six weeks when triggered, or may even go on for longer.
The illustration below illustrates the overall structure of the human vertebral column. Origin of pain could range from between the L4 (lumbar) region as far as the S1 (sacrum) region as all of these vertebrae have nerve roots that lead to the sciatic nerve.
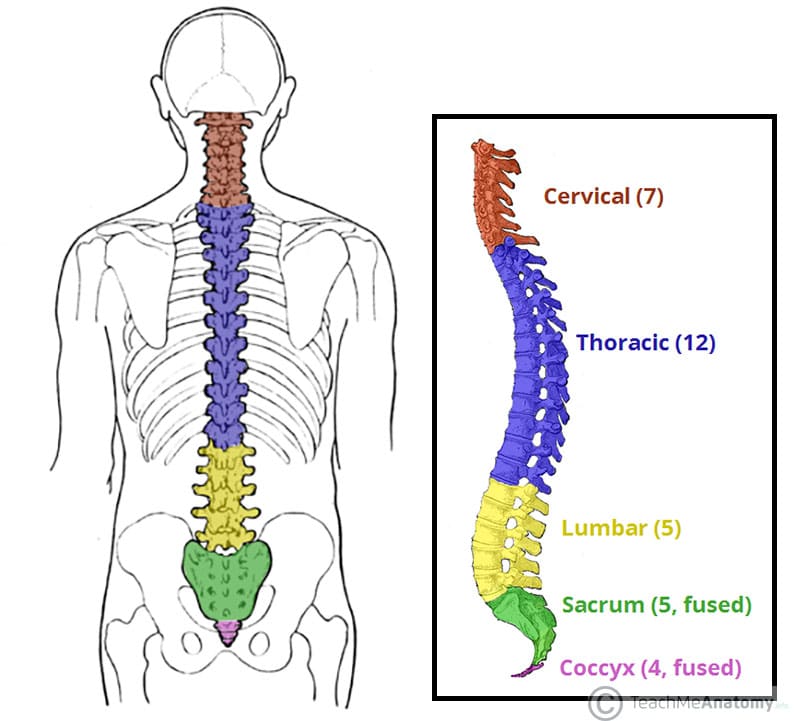
Illustration from TeachMeAnatomy
Symptoms
Sciatica may affect one or more parts of the lower limb corresponding to the sciatic nerve path including the buttock, hip, back of the leg (upper or lower), foot or even toes. Back pain is rare but not uncommon. More often than not, it affects one side of the body, but could also be symmetrical.
Manifestation of symptom(s) may vary between individuals or between episodes. These usually include one or more of the following:
- pain – intensity may vary from mild to sharp/burning pain
- numbness
- pins and needles sensation (tingling)
- feeling of weakness
Symptoms may be exacerbated by movement, reflex actions such as sneezing and coughing, or even remaining sedentary in a non-ideal posture/position.
Complications
Sciatica does not generally present with complications other than discomfort pertaining to movement and activity. However, depending on the severity of the cause of the condition, sciatica may be associated with weakness or complete loss of feeling in the affected leg and, on some occasions, loss of bladder or bowel control.
Causes
Following are a some of the possible causes of sciatica pain:
- herniated/slipped disc – This is the most common cause of sciatica. Vertebral discs are pads that lie between the vertebrae of the vertebral column (spine). They have a gel-like centre and act like a cushion, preventing friction between vertebrae and helping to keep them in place. In the event that the outer wall of a disc weakens, vertebral pressure can cause the gel-like centre to herniate (bulge out). If such herniation occurs in the lower back, it could press on the sciatic nerve and subsequently lead to sciatica.

Illustration from Mayo Foundation for Medical Education and Research
- spinal stenosis – The spinal canal is the space along the vertebral column through which the spinal cord passes. Abnormal narrowing of this canal, due to various reasons, could result in the sciatic nerve root being compressed, and subsequent sciatica.

Illustration from Cleveland Clinic
- degenerative disc disease – This is a natural process that occurs with age. Natural wear and tear of the discs reduces the cushioning between vertebrae, often leading to spinal stenosis and potentially causing sciatica.
- osteoarthritis – Bone spurs (jagged growths from the bone) from osteoarthritis or the aging process could also cause compression of the sciatic nerve.

Illustration from Mayo Foundation for Medical Education and Research
- spondylolisthesis – This occurs when a vertebra slips out of place, thereby narrowing the space available for the nerve to pass through.
- piriformis syndrome – The piriformis muscle connects the lower part of the vertebral column to the femur (thighbone) and helps with hip rotation. Inflammation or spasming of this muscle can exert pressure on the sciatic nerve, thereby causing sciatica.
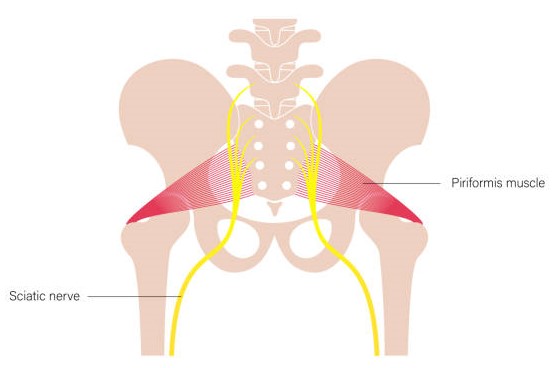
Illustration from iStock
- tumours – The presence or growth of benign or malignant tumours along the vertebral column may also cause compression of the sciatic nerve and subsequent sciatica.
- trauma – Traumatic incidents such as falls, pelvic fracture or dislocation, motor accidents, sports injuries, etc. can also cause compression or irritation of the sciatic nerve, leading to sciatica.
Sciatica may also be triggered during pregnancy in some cases as the weight gained exerts pressure on the lower spine of the mother.
Diagnosis
Sciatica can often be diagnosed by your doctor or physiotherapist by means of asking questions pertaining to your medical history and discomfort experienced, as well as assessment of your mobility such as walking, bending, lifting, weakness, reduced reflexes and the likes.
X-rays may be prescribed in the event of a suspected fracture, tumour or injury in the vertebral column or hip region. MRI or CT scans may be used to get a closer look at the affected area. Often, an MRI scan may be prescribed to confirm the diagnosis of the causal factor of sciatica.
Prevention
A few basic day-to-day measures that can be practised to avoid the incidence of sciatica include:
- maintaining good posture while sitting, sleeping, standing, lifting heavy objects
- maintaining a healthy weight so as not to exert excessive strain on the vertebral column
- exercising regularly to maintain strength and mobility in joints and muscles
- avoiding strenuous physical activity that could exert pressure on the back
- wearing well-fitted shoes when walking
- keeping your living and working spaces clutter-free to avoid falls
- not smoking so as not to hamper blood supply to bones (particularly of the vertebral column, in this case)
Treatment
With the right balance of rest and therapeutic exercise, sciatica can often be self-healing over a span of roughly four to six weeks. Physiotherapy may help to relieve some of the pain and discomfort, while self-care exercises may also be sought from a trained physiotherapist. In addition, prescribed anti-inflammatory drugs and painkillers may help to support alleviation of the symptoms.
In some cases, corticosteroid injections may be administered to relieve a patient of their pain. However, it is best to avoid this as much as possible due to the long-term after-effects of steroid administration. Relief may also only last for as long as the injection is effective, after which symptoms may re-emerge. If prescribed, not more than three corticosteroid injections should be administered within one year.
In extreme cases, particularly if there is loss of bladder/bowel control, surgery may be recommended to deal with conditions where other modes of treatment have failed. This may involve removal of spurs, microdisectomy (removal of a fragment of a herniated disc) or laminectomy (removal of the lamina part of a vertebra that is compressing the sciatic nerve). However, extra care should be taken as spinal surgery has a higher risk of causing other medical complications.
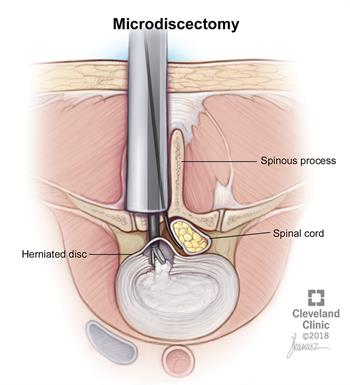
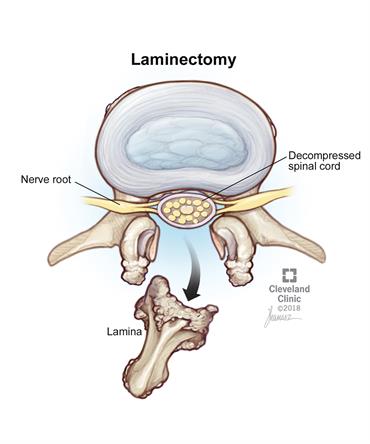
Illustrations from Cleveland Clinic
* ‘Disc’ is the preferred spelling in British English, whereas ‘disk’ is the preferred spelling in American English.
Cover illustration adapted from VectorStock
