Eyesight/vision is one of our five senses that we largely rely on for basic survival and day-to-day navigation. The image below shows the structure of the eye.
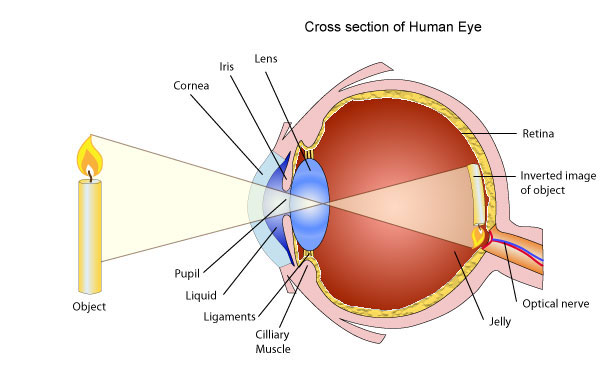
Our vision is determined by the collective function of different parts of the eye. Light from an object that enters through the clear, dome-shaped cornea passes through the pupil and is selectively allowed in through the iris (the coloured part of our eye). This then passes through the lens which focuses the light onto the retina. The retina’s photoreceptor cells turn this light into electric signals which are transmitted to the brain via the optic nerve. The brain then makes sense of these signals and gives us a visual of the object.
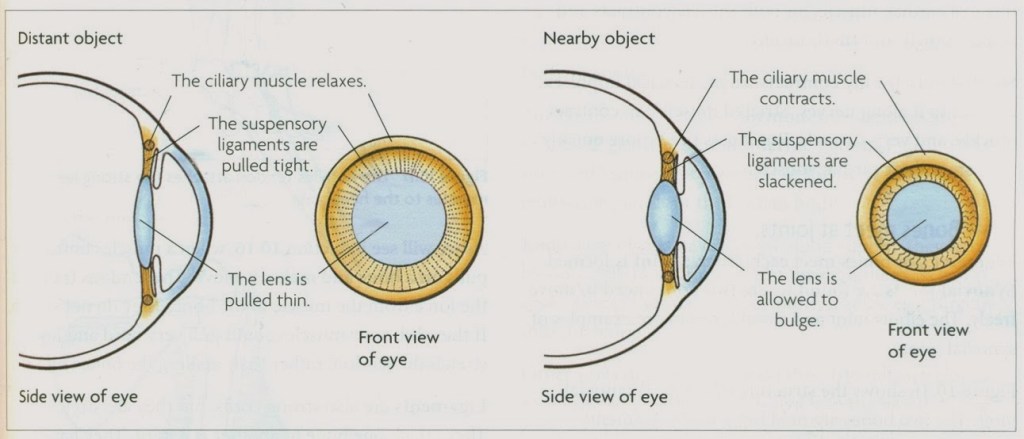
With the help of the eye muscles and ligaments, the lens is pulled thin when focusing light from distant objects, and allowed to thicken when focussing light from nearby objects.
Symptoms
| Myopia | Hyperopia |
| Myopia is often diagnosed between the ages of 6-13 years. In younger children who may not be able to express or realise a difference in sight, a few signs to look out for include: · difficulty reading the board in school, so needing to sit at the front of the class · needing to sit close to the screen when watching television · complaints of headaches · complaints of feeling tiredness in eyes regular rubbing of eyes | Individuals with hyperopia, or long-sightedness, can usually see distant objects clearly, while nearby objects appear out of focus. However, sometimes, overall vision (i.e. both near and far) may be unclear. While it may occur at any age, hyperopia is most commonly prevalent in people over the age of 40 years. Symptoms include: · feeling strain or tiredness in eyes after doing work that requires focus on nearby objects · having to squint to see clearly · frequent headaches |
Complications
| Myopia | Hyperopia |
| In cases where short-sightedness is severe or left untreated, there is a possibility of developing one or more of the following complications: · lazy eye, where one eye’s vision is underdeveloped (in childhood) · squint, where the eyes point in different directions (in childhood) · cataract, where the lens develops cloudy patches · glaucoma, where eye pressure increases retinal detachment, where the retina pulls away from blood vessels, starving the eye of oxygen and nutrients | Children with untreated hyperopia may develop either of the following complications: · lazy eye, where one eye’s vision is underdeveloped · squint, where the eyes point in different directions |
Causes
| Myopia | Hyperopia |
| Myopia usually occurs when the eyeball grows longer (back to front) than it should normally be. As such, light from distant objects gets focussed in front of the retina rather than on it. The resulting image is blurry. Although it is not certain as to why this phenomenon occurs, there are several factors that seem to increase the risk: · genetics, where likelihood for myopia is greater where there is a family history · excessive time spent focussing on nearby objects such as books (reading/writing), computer screens, phones and tabs, etc. insufficient time spent outdoors during childhood (e.g. for sport, leisure), possibly due to natural outdoor light being brighter than indoor light | In hyperopia, the eyeball length is shorter than should ideally be. Hence, light from a given object does not focus on the retina, and is projected to focus behind it instead. As with myopia, the reasons for hyperopia are not certain, however risk factors appear to be: · genetics, where likelihood for hyperopia is greater where there is a family history · the lens not being able to focus light properly onto the retina · the cornea being too flat |
Diagnosis
The most straight-forward means of testing your visual acuity is by means of using an eye chart – the most common of which is the Snellen Eye Chart. This comprises a chart of letters which decrease in size from top to bottom. It is placed six feet away from the patient, from which distance they are asked to read selected or all letters. This is usually done separately for each eye, as well as with and without spectacles, if the patient wears spectacles.

Image from Hopkins Medical Products
Depending on necessity, your ophthalmologist may also:
- measure your eye pressure (drops may be administered for pupil dilation, about 15-30 minutes prior to examination)
- check how well your eyes work in tandem
- check on how your eye reacts to bright light in a test referred to as retinoscopy
These tests may individually or collectively enable the diagnosis of myopia or hyperopia, in which case the ophthalmologist will record three significant indicators on your prescription for spectacles or lenses:
- sphere (Sph) – measured in dioptres (D), where a negative value indicates myopia and a positive value indicates hyperopia (-0.5D to -3D / 0.5D to 3D is considered mild, while beyond -6D / 6D is considered severe)
- cylinder (Cyl) – an indication of whether astigmatism (imperfect curvature of the cornea) is present or not
- axis – measure of the angle of astigmatism, if present
Prevention
There is no certain means of preventing myopia or hyperopia. However, the following measures could be practised for precaution and to maintain good eye health:
- make a habit of getting your eyes tested every two years
- do eye exercises that stretch and relax the lens and associated muscles and ligaments (e.g. focus on a pencil point as you slowly move it away from and towards your face alternatingly, at eye level; also, move eyeballs from side to side and in up-down and circular motions while keeping your head still)
- incorporate vitamin A-rich foods (e.g. carrot, sweet potato, spinach, broccoli, cod liver oil, black-eyed peas) into your diet regularly
- follow the 20-20 eye care routine – for every 20 minutes of screen time, look away and relax your eyes for 20 seconds
- avoid prolonged periods of focusing on nearby objects (e.g. screens, books) – this might specially be beneficial against myopia
Treatment
Following are a few common methods of treatment used to improve vision:
- spectacles/glasses, which are the most common form of treatment. Lenses should be made to the ophthalmologist’s specifications, and may be prescribed long-term, or as a short-term corrective measure. Older patients may require two pairs – one for close proximity and the other for distance. Alternatively, both lens specifications may be modelled into a single pair in the form of bifocal (or sometimes multifocal) lenses.
- contact lenses, which follow the same as glasses in terms of being prescription-specific, and long-term or corrective.
- laser eye surgery, where laser is used to burn and adjust the curvature of the cornea to allow light to be focused better on the retina. This is usually an out-patient procedure and may be any one of photorefractive keratectomy (PRK), laser epithelial keratomileusis (LASEK) or laser in situ keratectomy (LASIK). Which of these procedures best suits you should be discussed with your ophthalmologist.
Cover illustration adapted from Ya-Webdesign.
